Pulse wave and vascular age — Arteries expire, too
Pulse Wave and Biological Age
Arteries expire, too
Arteries transport oxygen-rich blood from the heart throughout the body. If you are young and healthy, your blood vessels are wide enough in diameter to allow blood to flow easily through them. At this point, the arterial walls are still flexible enough to expand and contract as needed and can easily absorb the hard pressure shocks of the heart.
As we age, the arteries harden and lose flexibility: plaque — consisting of cholesterol, fat, calcium, and fibrous tissue — builds up inside, and the vessels become increasingly narrow. This process, known as atherosclerosis, is associated with a high risk of heart attacks, strokes, and peripheral artery disease (PAD): Arterial aging begins much earlier than most would think.
How arteries age
“Atherosclerosis usually begins in the teens and 20s, and by age 30, we can see changes in most people,” says cardiologist Matthew Sorrentino MD, professor at the University of Chicago Medicine’s Bucksbaum Institute for Clinical Excellence. In the early stages, results of heart-related screening tests, such as cholesterol screenings, are usually still considered normal.
However, as people age, the problem usually gets worse: By age 40, about half of us have cholesterol deposits in our arteries, Sorrentino says. After age 45, men have numerous plaque deposits in their blood vessels. In women, the first signs of atherosclerosis usually appear after age 55.
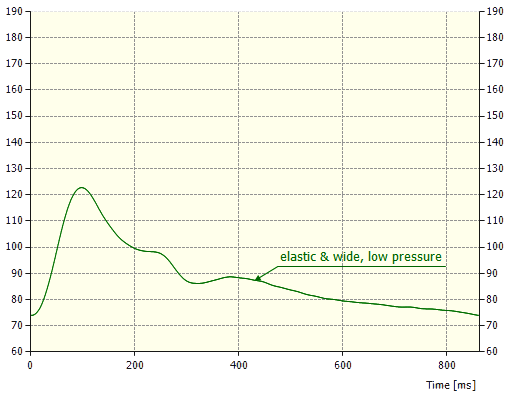
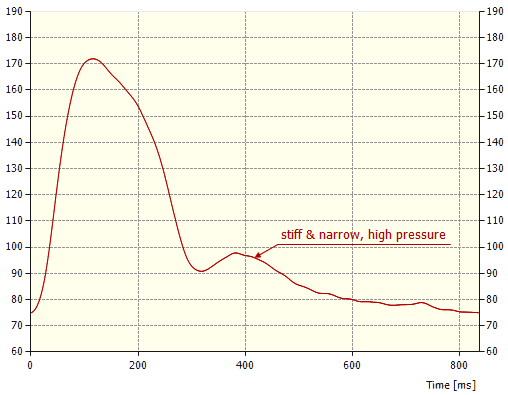
Comparison of the radial pulse waves of two 55-year-old men — at the same scaling.
The green curve is age-appropriate in its progression. In contrast, the red curve shows the grave difference between the patient’s vascular and actual age: The elasticity of the arteries of the 55-year-old man corresponds to that of an 80-year-old, and the flow resistance to that of a 75-year-old.
Risk Factors and Associated Conditions
It’s not just age that affects the arteries. Lifestyle also plays a role: obesity, smoking, lack of exercise, and consumption of foods high in dangerous trans fats exert an influence on the condition of the vessels. Added to this is family history and, thus, genetic factors. As a result, some people experience chest pain, fatigue, or shortness of breath in the later stages of atherosclerosis. Some, however, do not notice any symptoms.
All the more important is to assess the likelihood of developing the accompanying symptoms of aged arteries, Sorrentino says. Various factors play a role in risk assessment. For example, cholesterol levels and other specific markers in the blood count are included in the evaluation, as is weight and, of course, the entire medical and family history. The linchpin of an individual risk profile, however, is to determine the hemodynamic properties of the arteries. Central and peripheral blood pressure measurements based on Model-based Pulse Wave Analysis (mbPWA) identify the likelihood of an emergency, such as a heart attack or stroke, in the next few years. It also unequivocally determines the likelihood of peripheral vascular occlusion (arms or legs) at a very early (often still asymptomatic) stage.
Protect yourself from atherosclerosis
Although you can’t change your actual age or family history, being proactive is crucial to keeping your arteries healthy for as long as possible.
Take regular exercise, eat a balanced diet, lose excess pounds, and don’t smoke, says Sorrentino.
Also always advisable is a visit to the doctor to clarify whether there is a risk of atherosclerosis. Sometimes, effective lifestyle changes like Sorrentino recommends are all needed. In the case of advanced atherosclerosis, depending on the individual patient, it is recommended to take medication to reduce the risk of a heart attack or stroke.

